
Have you ever wondered why some people develop diabetes despite maintaining a healthy weight and active lifestyle, while others develop the condition primarily due to lifestyle factors? Why do some people with diabetes absolutely require insulin from day one, while others may never need insulin injections? How can two conditions that share the same name—diabetes—require such radically different approaches to management? The answers lie in understanding the fundamental differences between Type 1 and Type 2 diabetes.
Though both conditions involve problems with insulin and blood glucose regulation, they differ dramatically in their underlying mechanisms. Is your pancreas unable to produce insulin due to an autoimmune attack (Type 1), or is your body resistant to the insulin it produces (Type 2)? At IFitCenter, we’ll explore these essential distinctions that affect millions worldwide. Understanding which type of diabetes you have—and its specific characteristics—is the first step toward effective management. In this comprehensive guide, we’ll answer these challenging questions and provide clarity on how these two conditions differ at their very core.
Root Causes of Diabetes Types
To understand the fundamental differences between Type 1 and Type 2 diabetes, we must first grasp how insulin normally works in the body and what goes wrong in each condition.
“Many patients are surprised to learn that Type 1 and Type 2 diabetes involve entirely different cellular mechanisms. In Type 1, we’re seeing an autoimmune cascade that destroys beta cells, while in Type 2, the insulin receptors on cells throughout the body gradually lose their sensitivity long before blood glucose rises significantly. Understanding this distinction explains why the treatment approaches differ so dramatically and why lifestyle modifications that are powerfully effective for Type 2 may have minimal impact on insulin requirements for Type 1.”
Dr. Babak Jamalian, Family Physician.
The Insulin-Glucose Relationship: Your Body’s Energy System
Imagine your bloodstream as a vast delivery network and glucose (sugar) as the primary fuel packages that power your cells. After you eat, your food breaks down into glucose, which enters your bloodstream. However, this glucose can’t simply drift into your cells on its own—it needs a key to unlock the cell doors.
This is where insulin comes in. Produced by specialized beta cells in your pancreas, insulin acts like a key that opens cellular “doors” called receptors. When insulin binds to these receptors, it allows glucose to enter the cell where it can be used for energy. Without this key, glucose remains trapped in your bloodstream, unable to fuel your body’s functions.
In a healthy body, this system maintains a delicate balance: when blood glucose rises, the pancreas releases just enough insulin to move that glucose into cells, keeping blood sugar levels within a narrow, healthy range. Once glucose enters the cells, insulin levels decrease until the next meal.
Type 1 Diabetes: When the Insulin Factories Shut Down
Type 1 diabetes represents a case of mistaken identity within your immune system. In this condition, the body’s immune defenses—which normally protect against harmful invaders like bacteria and viruses—incorrectly identify the insulin-producing beta cells in the pancreas as foreign threats and systematically destroy them.
This autoimmune attack is like sabotage at the insulin factory. As beta cells are destroyed, insulin production decreases until eventually, little to no insulin is made. Without the key, glucose cannot enter cells, leading to high blood sugar levels despite cells essentially starving for energy. Unlike many health conditions that develop gradually, this autoimmune destruction can progress rapidly, especially in children and adolescents, which explains why Type 1 diabetes often appears suddenly and dramatically.
Once this autoimmune process starts, it typically continues until nearly all beta cells are destroyed. Since these specialized cells cannot regrow or regenerate in significant numbers, the body loses its ability to produce insulin—permanently. This is why people with Type 1 diabetes require external insulin from the moment of diagnosis and for the rest of their lives.
Type 2 Diabetes: When the Keys Stop Working
In stark contrast to Type 1, Type 2 diabetes typically begins not with destruction of beta cells but with a phenomenon called insulin resistance. Imagine the cell doors gradually changing their locks over time so that the insulin keys no longer fit perfectly. The keys (insulin) still exist, but they become less effective at opening the doors.
Initially, the pancreas compensates by producing more insulin—essentially making more keys in hopes that some will work. This compensatory mechanism can work for years or even decades, which explains why many people with insulin resistance don’t immediately develop diabetes. However, this overproduction places enormous stress on the beta cells.
Eventually, after years of overwork, the pancreas’s beta cells become exhausted and begin to fail. It’s like a factory running triple shifts for years—eventually, the machinery breaks down. As beta cell function declines, insulin production decreases despite the body’s increased needs. This creates a double problem: not enough keys (insulin) and locks that don’t work well (insulin resistance).
Unlike the rapid onset seen in Type 1 diabetes, Type 2 diabetes develops gradually. Blood glucose levels rise slowly over time, often without noticeable symptoms until the condition is quite advanced. This is why Type 2 diabetes is frequently discovered during routine medical tests rather than from acute symptoms.
Take Control of Type 2 Diabetes Through Weight Management
Type 2 diabetes often begins silently, gradually driven by weight gain, insulin resistance, and lifestyle habits. But here’s the good news: managing your weight can significantly improve your body’s insulin sensitivity and help maintain balanced blood sugar levels.
At iFitCenter, we offer medically supervised, personalized weight management programs designed specifically for those with insulin resistance or Type 2 diabetes. By starting with a detailed metabolic evaluation, we create tailored nutrition and weight-loss plans to effectively address the root causes of your condition, helping you achieve lasting health and metabolic balance.
If you’re ready to take proactive steps toward controlling your diabetes through sustainable weight management, our medical team is here to guide you.
Genetic and Environmental Influences: Why Do These Changes Occur?
Both types of diabetes involve a complex interplay between genetic predisposition and environmental factors, though in different ways.
In Type 1 diabetes, genetic factors create vulnerability to the autoimmune process. Certain genes, particularly those in the HLA complex (which helps the immune system distinguish between self and non-self), play a significant role. However, genetics alone isn’t enough—environmental triggers are needed to initiate the autoimmune attack. These may include viral infections, early diet influences, or other environmental factors not yet fully understood.
For Type 2 diabetes, genetic predisposition is even stronger—having a parent or sibling with Type 2 diabetes significantly increases your risk. However, lifestyle factors play a critical role in whether these genetic tendencies manifest as disease. Physical inactivity, excess body weight (especially around the abdomen), and dietary choices can all contribute to insulin resistance, while aging also increases vulnerability.
Interestingly, Type 2 diabetes risk varies among different ethnic groups, with higher rates among people of Middle Eastern, African, Hispanic, and South Asian descent, suggesting strong genetic components influenced by evolutionary adaptations to different environments and food availability.
Understanding these fundamental differences in causation is essential for proper management. Type 1 diabetes requires immediate and lifelong insulin replacement, while Type 2 often begins with lifestyle modifications aimed at reducing insulin resistance, and may progress to requiring medications or insulin as beta cell function declines over time.
Diagnosing Different Diabetes Types
Correctly identifying which type of diabetes someone has is crucial for determining the right treatment approach. While both types share the common feature of elevated blood glucose, their diagnostic pathways often differ significantly.
On the IFitCenter blog, we have provided a comprehensive guide for diabetes, completely free of charge and based on the latest research. By viewing these articles, in addition to increasing your general knowledge in this field, you can easily manage this disease in a principled manner. To access the first part of the articles, simply use the links below:
- What is Diabetes?
- Symptoms and Signs of Diabetes
- What Are the Complications of Diabetes?
- Diabetes Diagnosis Method
- Is Diabetes Curable?
Key Diagnostic Criteria and Blood Glucose Thresholds
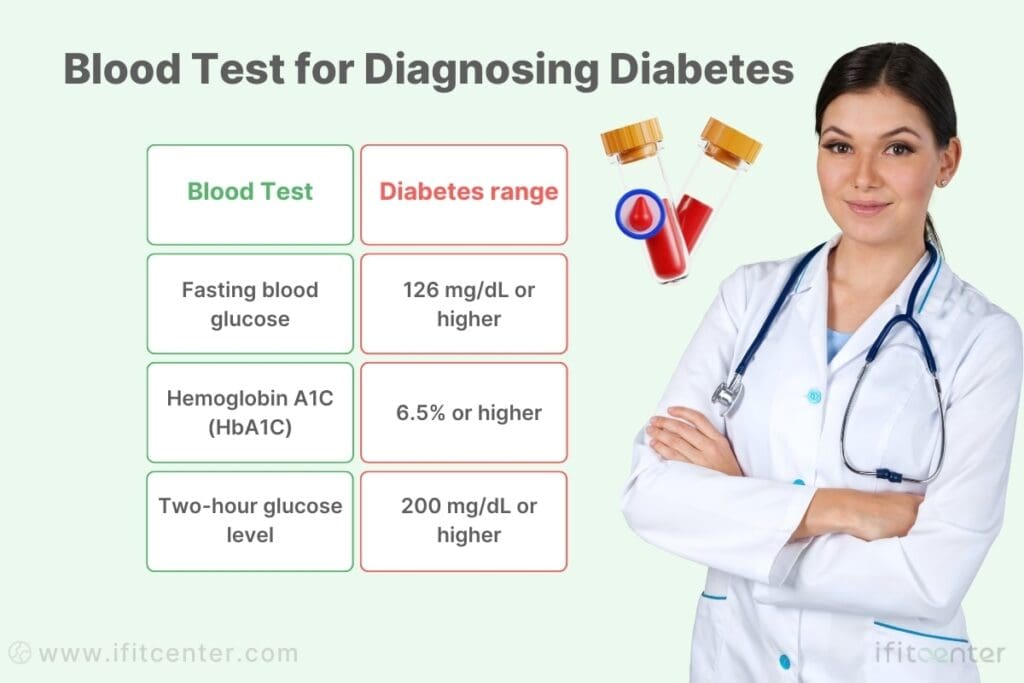
Regardless of type, diabetes diagnosis relies on specific blood glucose thresholds. A diagnosis can be made when any of these criteria are met:
- Fasting blood glucose level of 126 mg/dL (7.0 mmol/L) or higher
- Two-hour glucose level of 200 mg/dL (11.1 mmol/L) or higher during an oral glucose tolerance test
- Random blood glucose level of 200 mg/dL (11.1 mmol/L) or higher in a person with classic symptoms
- Hemoglobin A1C of 6.5% or higher
However, while these thresholds determine whether someone has diabetes, they don’t specify which type. For that, healthcare providers must look deeper at other factors and additional tests.
Age and Presentation Patterns That Provide Clues
The age at diagnosis and the pattern of symptom onset often provide the first clues to diabetes type:
Type 1 diabetes typically presents with:
- More common in children and young adults, though it can develop at any age
- Sudden and severe symptom onset, often developing over days or weeks
- Significant weight loss despite normal or increased appetite
- Pronounced thirst and frequent urination
- Often presents with diabetic ketoacidosis (DKA), a serious condition requiring emergency treatment
Type 2 diabetes typically presents with:
- More common in adults over 40, though increasingly seen in younger populations
- Gradual symptom development, sometimes with no noticeable symptoms for years
- Often associated with excess weight, especially around the abdomen
- Frequently discovered during routine blood tests rather than from symptoms
- Rarely presents with ketoacidosis unless complicated by severe illness
Essential Tests for Accurate Classification
Beyond basic glucose testing, several specific tests help differentiate between diabetes types:
Autoantibody Testing: The presence of certain autoantibodies in the blood indicates the autoimmune process of Type 1 diabetes. These include:
- Islet cell autoantibodies (ICA)
- Glutamic acid decarboxylase autoantibodies (GADA or anti-GAD)
- Insulin autoantibodies (IAA)
- Insulinoma-associated-2 autoantibodies (IA-2A)
C-peptide Test: This measures how much insulin your body produces naturally. People with Type 1 diabetes typically have very low or undetectable C-peptide levels, while those with Type 2 often have normal or high levels, especially early in the disease.
Insulin Resistance Assessment: Various methods can help determine the degree of insulin resistance, which is characteristic of Type 2 diabetes. These include fasting insulin levels and more complex assessments like the HOMA-IR calculation.
Risks of Misdiagnosis and Their Consequences
Misclassification of diabetes type can have serious consequences:
If Type 1 is mistaken for Type 2:
- Delay in insulin therapy, which is essential for survival
- Increased risk of diabetic ketoacidosis, a life-threatening condition
- Improper treatment approach focusing on reducing insulin resistance rather than replacing missing insulin
If Type 2 is mistaken for Type 1:
- Unnecessary insulin therapy when oral medications might be effective
- Missed opportunities to address underlying insulin resistance through lifestyle modifications
- Different monitoring and education needs than what may be appropriate
Interestingly, some adults are initially misdiagnosed with Type 2 diabetes when they actually have a slow-progressing form of Type 1, sometimes called Latent Autoimmune Diabetes in Adults (LADA). These individuals may initially respond to Type 2 treatments but eventually require insulin as their autoimmune process continues to destroy beta cells.
The key takeaway is that proper diabetes classification requires more than just measuring blood glucose. Understanding the underlying mechanisms—autoimmune destruction versus insulin resistance—is essential for appropriate treatment and management strategies. If you have any doubts about your diabetes diagnosis, discussing additional testing with your healthcare provider could provide valuable clarity.
Symptoms: Type 1 vs. Type 2 Diabetes
The symptoms of diabetes result from high blood glucose levels, but the pattern and intensity of these symptoms differ markedly between Type 1 and Type 2 diabetes. Recognizing these differences can be crucial for timely diagnosis and appropriate treatment.
Common Symptoms in Both Diabetes Types
Despite their different origins, both types of diabetes share several core symptoms caused by elevated blood glucose:
- Polydipsia (excessive thirst) – As your body tries to flush out excess glucose through urine, you become dehydrated and thirsty
- Polyuria (frequent urination) – High blood glucose levels force your kidneys to work overtime to filter and absorb the excess glucose
- Polyphagia (increased hunger) – Despite having high blood glucose, your cells are starving for glucose they cannot access
- Fatigue – When cells cannot use glucose for energy, you feel constantly tired
- Blurred vision – High glucose levels can affect fluid levels in your eye lenses, temporarily changing their shape
Type 1 Diabetes: Rapid and Dramatic Symptom Onset
Type 1 diabetes typically presents with distinct characteristics that reflect the sudden loss of insulin production:
- Sudden symptom development – Symptoms often appear and intensify over days or weeks, not months or years
- Unexplained weight loss – Despite normal or even increased eating, significant weight loss occurs as the body breaks down fat and muscle for energy
- Intense thirst and frequent urination – These symptoms are often dramatic and disruptive
- Stomach pain, nausea, or vomiting – Particularly when ketones build up in the bloodstream
- Fruity-smelling breath – A sign of ketones in the body
- Mood changes and irritability – Often notable, especially in children
These symptoms typically appear rapidly because the autoimmune destruction of beta cells reaches a critical threshold where insulin production suddenly becomes insufficient for the body’s needs.
Type 2 Diabetes: The Silent Progression
In stark contrast to Type 1, Type 2 diabetes often develops so gradually that symptoms may go unnoticed for years:
- Gradual symptom development – Symptoms typically develop slowly, sometimes over several years
- Subtle thirst and urination changes – Less dramatic than in Type 1, making them easier to dismiss
- Recurring infections – Particularly urinary tract infections, yeast infections, and skin infections
- Tingling or numbness in extremities – Due to early nerve damage from sustained mild hyperglycemia
- Dark patches of skin – Particularly in body folds like the neck and armpits (acanthosis nigricans), indicating insulin resistance
- Increased fatigue after meals – Especially carbohydrate-rich meals
- Slow-healing sores – Elevated blood glucose impairs circulation and immune response
Many people with Type 2 diabetes remain undiagnosed for years because symptoms develop so gradually they’re often attributed to aging or stress. This silent progression allows damage to occur before diagnosis.
When Diabetes Symptoms Signal an Emergency
Certain diabetes symptoms require immediate medical attention:
- Diabetic ketoacidosis (DKA) – Common in Type 1 and characterized by fruity breath, deep labored breathing, confusion, extreme thirst, and high blood glucose levels
- Hyperosmolar hyperglycemic state (HHS) – More common in Type 2 and marked by extreme dehydration, confusion, very high blood glucose (often over 600 mg/dL), and no ketones
- Severe dehydration – Evidenced by extreme thirst, dry mouth, sunken eyes, and confusion
- Severe hypoglycemia – In diagnosed diabetes patients who take medications, symptoms include shakiness, confusion, seizures, or loss of consciousness
These emergency conditions require immediate medical intervention and can be life-threatening if not treated promptly.
Treatment Differences by Diabetes Type
The fundamental differences between Type 1 and Type 2 diabetes necessitate distinct treatment approaches. These differences affect everything from medication needs to lifestyle recommendations.
To access the second part of the articles related to diabetes, you can use the following links:
- The Difference Between Prediabetes and Diabetes
- Insulin Resistance and Diabetes
- Understanding Blood Sugar Numbers
- Weight Loss for Type 2 Diabetes
- Causes of Diabetes
- How can I prevent diabetes naturally
- How to take apple cider vinegar to lower blood glucose
Insulin Therapy: Necessity vs. Possibility
In Type 1 diabetes, insulin therapy isn’t just a treatment option—it’s a survival requirement. Since the body can no longer produce insulin, external insulin must be provided immediately upon diagnosis and continued for life. Without insulin, a person with Type 1 diabetes cannot process glucose and will develop life-threatening complications within days.
For Type 2 diabetes, insulin therapy follows a different pattern. Initially, many people with Type 2 can manage their condition through lifestyle changes and oral medications. Insulin becomes necessary only when these approaches no longer maintain adequate blood glucose control—typically when beta cell function has significantly declined. This might occur immediately in some cases but may take years or decades in others.
Medication Options Specific to Each Type
Type 1 diabetes treatment relies primarily on insulin, with few other medication options. The focus is on matching insulin delivery to carbohydrate intake and activity levels. Multiple insulin types may be used together to mimic natural insulin patterns:
- Rapid-acting insulin for mealtime glucose spikes
- Long-acting insulin for background glucose control
Type 2 diabetes offers a much broader medication landscape:
- Metformin – Usually the first medication prescribed, it reduces glucose production by the liver
- SGLT-2 inhibitors – Help the kidneys remove glucose through urine
- GLP-1 receptor agonists – Slow digestion and help reduce appetite while stimulating insulin release
- DPP-4 inhibitors – Help increase insulin production and decrease liver glucose production
- Sulfonylureas – Stimulate the pancreas to release more insulin
- Thiazolidinediones – Reduce insulin resistance
These medications target different aspects of Type 2 diabetes pathology, often working in combination to achieve optimal blood glucose control.
“One of the most significant recent advances in diabetes care is our understanding that different medication classes have benefits far beyond glucose control. For example, SGLT-2 inhibitors reduce hospitalization for heart failure by approximately 30% in Type 2 diabetes patients, while GLP-1 receptor agonists specifically reduce the risk of non-fatal stroke. This research has completely transformed our approach from simply targeting glucose numbers to selecting medications based on a patient’s specific cardiovascular and kidney risk profiles.”
Dr. Babak Jamalian, Family Physician.
Dietary Approaches for Different Diabetes Types
While healthy eating benefits all types of diabetes, specific dietary approaches differ:
For Type 1 diabetes, dietary management centers on:
- Carbohydrate counting to match insulin doses
- Consistent meal timing to work with insulin action
- Learning how different foods affect individual blood glucose responses
For Type 2 diabetes, dietary approaches focus on:
- Reducing overall carbohydrate intake, particularly refined carbohydrates
- Weight management if overweight or obese
- Portion control and calorie awareness
- Including foods that minimize blood glucose spikes
Low-carbohydrate and ketogenic approaches have shown particular promise for Type 2 diabetes, potentially reducing medication needs and improving metabolic health markers.
Exercise Considerations: Different Impacts by Type
Physical activity benefits both diabetes types but requires different management approaches:
For Type 1 diabetes, exercise management involves:
- Adjusting insulin doses before, during, and after activity
- Monitoring blood glucose more frequently during exercise
- Having fast-acting carbohydrates readily available to prevent hypoglycemia
- Understanding that different exercise types affect blood glucose differently
For Type 2 diabetes, exercise considerations include:
- Using exercise as a primary treatment to reduce insulin resistance
- Combining both aerobic exercise and resistance training for optimal results
- Monitoring potential medication adjustments as fitness improves
- Consistent activity rather than occasional intense sessions
Monitoring Requirements and Technologies
Blood glucose monitoring needs differ significantly between diabetes types:
Type 1 diabetes typically requires:
- More frequent daily glucose monitoring (often 4-10 times daily)
- Greater use of continuous glucose monitoring systems
- Careful tracking of insulin doses, carbohydrates, and activity
- Regular monitoring for ketones when blood glucose is elevated
Type 2 diabetes monitoring often involves:
- Less frequent daily glucose checks (typically 1-2 times daily)
- Periodic A1C testing to assess long-term control
- Tracking of weight and other metabolic markers
- Adjustment of monitoring frequency based on medication types
Understanding these treatment differences highlights why proper diabetes classification is so crucial. Misclassification can lead to inappropriate treatment strategies that fail to address the underlying metabolic problems, potentially resulting in poor outcomes and unnecessary complications.
What’s the Difference Between Type 1 and Type 2 Diabetes
Throughout this article, we’ve explored the crucial distinctions between Type 1 and Type 2 diabetes—conditions that share a name but differ fundamentally in their causes, progression, and management approaches.
Type 1 diabetes results from an autoimmune attack that destroys insulin-producing cells, creating an absolute insulin deficiency that requires lifelong insulin therapy. It typically appears suddenly with pronounced symptoms and can affect people at any age, though it’s often diagnosed in childhood or adolescence.
In contrast, Type 2 diabetes develops from a combination of insulin resistance and progressive beta cell dysfunction. This gradual process often allows the condition to develop silently for years before diagnosis. While genetics play a role in both types, Type 2 is significantly influenced by lifestyle factors, creating more opportunities for prevention and sometimes partial reversal.
These foundational differences explain why treatment approaches vary so dramatically. While insulin is immediately necessary for survival in Type 1 diabetes, Type 2 management often begins with lifestyle modifications and oral medications, with insulin becoming necessary only as beta cell function declines over time.
Understanding your specific diabetes type is essential for appropriate management. Each person’s diabetes experience is unique, requiring a personalized approach that addresses their particular metabolic profile, lifestyle factors, and health goals. One-size-fits-all recommendations rarely produce optimal results in such a complex condition.
To access other content on the IFitCenter’s blog, you can use the following links:
References for Type 1 and Type 2 Diabetes Difference
- Madurapperumage Anuradha Erandathi, William Yu Chung Wang, Michael Mayo, Ching-Chi Lee. Comprehensive Factors for Predicting the Complications of Diabetes Mellitus: A Systematic Review. Curr Diabetes Rev. 2024;20(9):e040124225240. DOI: 10.2174/0115733998271863231116062601
- Matti Uusitupa, Tauseef A Khan, Effie Viguiliouk, Hana Kahleova, Angela A Rivellese, Kjeld Hermansen, Andreas Pfeiffer, Anastasia Thanopoulou, Jordi Salas-Salvadó, Ursula Schwab, John L Sievenpiper. Prevention of Type 2 Diabetes by Lifestyle Changes: A Systematic Review and Meta-Analysis. Nutrients. 2019;11(11):2611. DOI: 10.3390/nu11112611
- Karla Ivette Galaviz, Mary Beth Weber, Audrey Straus, Jeehea Sonya Haw, KM Venkat Narayan, Mohammed Kumail Ali. Global Diabetes Prevention Interventions: A Systematic Review and Network Meta-analysis of the Real-World Impact on Incidence, Weight, and Glucose. Diabetes Care. 2018;41(7):1526–1534. DOI: 10.2337/dc17-2222
- Annika Rosengren, Pigi Dikaiou. Cardiovascular outcomes in type 1 and type 2 diabetes. Diabetologia. 2023;66(3):425–437. DOI: 10.1007/s00125-022-05857-5
- Weronika Bielka, Agnieszka Przezak, Andrzej Pawlik. The Role of the Gut Microbiota in the Pathogenesis of Diabetes. Int. J. Mol. Sci. 2022;23(1):480. DOI: 10.3390/ijms23010480
- Danijela Tatovic, Ashish Marwaha, Peter Taylor, Stephanie J. Hanna, Kym Carter, W. Y. Cheung, Steve Luzio, Gareth Dunseath, Hayley A. Hutchings, Gail Holland, Steve Hiles, Greg Fegan, Evangelia Williams, Jennie H. M. Yang, Clara Domingo-Vila, Emily Pollock, Muntaha Wadud, Kirsten Ward-Hartstonge, Susie Marques-Jones, Jane Bowen-Morris, Rachel Stenson, Megan K. Levings, John W. Gregory, Timothy I. M. Tree; USTEKID Study Group. Ustekinumab for type 1 diabetes in adolescents: a multicenter, double-blind, randomized phase 2 trial. Nature Medicine. 2024;30:2657–2666. DOI: 10.1038/s41591-024-03115-2
- Hao Liu, Jianguo Feng, Liling Tang. Early renal structural changes and potential biomarkers in diabetic nephropathy. Frontiers in Physiology. 2022;13:1020443. DOI: 10.3389/fphys.2022.1020443



{kind=link}